Dr. James Lyons Weiler on the fake science of Measles vaccines
To the uninitiated, it must be nice to listen to so-called experts like CHOP’s Paul Offit discuss the science that supports the idea that vaccines are mostly safe – and by mostly they mean by far safe for everyone or nearly everyone. To hear such platitudes being described as “the strongest science shows the vaccines are perfectly safe” must be very reassuring indeed.
Unfortunately, the people who speak these phrases are fully aware that the epidemiological studies that are conducted to determine whether a vaccine has adverse events in the population are just about the weakest type of studies that can be conducted to detect adverse events that happen in a minority of patients. Ecological correlations (association tests) fall short of testing causality, so positive results can be rejected as “just correlations”. If that’s the case, negative results do not amount to a critical test of causality – not even close, especially when they are severely underpowered.
In reality, when adverse events happen in the population and weak and malleable and underpowered epidemiologic studies fail to detect an association the status of the inference is “No evidence”. The “no evidence” handle, however, has been conscripted at times: it has been used to make the claim of no causality, when in fact, not even a single study to test even for a particular association has been conducted.
It is rather psychotic to see particular types of adverse events happening after vaccination and to deny absolutely that the vaccination was (even in part) responsible simply because no association can be detected in larger association studies Here’s why:
First of all, the studies that have been conducted have never accounted for genetic differences that exist among the population that might put different individuals at risk of serious or moderate adverse events for vaccines. Not everyone can tolerate certain kinds of chemotherapy agents and therefore it would be a bit psychotic to say that a chemotherapy agent is perfectly safe even though we see people get sick and die rapidly on the chemo from the effects of chemo even though no known association has been found of those effects in an epidemiological study because we know that we have not yet tested those individuals for their tolerance of, let’s say, metals in the chemotherapy agent.
More importantly, though is the question of how senseless and utterly self-defeating vaccine injury and vaccine death denial is. Imagine a farmer who, once a year, goes to his fields and purposely sows seeds – not of his crops, but of wildflowers. The next season, when he sees what to him appear to be weeds growing in number, he (1) denies they are caused by him sowing the seeds, and then (2) blames the wildflowers themselves for being there. His solution? To sow more wildflower seeds, and wait until “one day” when his genius solution will convince everyone, including the wildflowers, that they are, in fact, not growing.

In the pre-vaccine era, the population of the US was about 180 million. According to the best available data, the number of deaths due to measles infection was between 450-500 deaths per year. Simple math tells us that’s a whole-population mortality rate of 0.00000278 – hardly a cause for alarm. In fact, the rate is so low that a whole-population cohort study would have a difficult time detecting a significant association between measles infection (which was common) and mortality, especially if, as CDC insists for studying autism, other risk factors for death due to measles infection like poor nutrition or body weight had to be adjusted for as ‘confounders’.
This report from Harvard University in 2001 shows just how little impact the measles vaccination program had on mortality due to measles infection. In their graph, shown below, the relative contribution of measles – prior to any vaccination program – was negligible. The measles vaccine is seen here clearly to be a Johnny-come-lately factor in reducing mortality from measles infection.
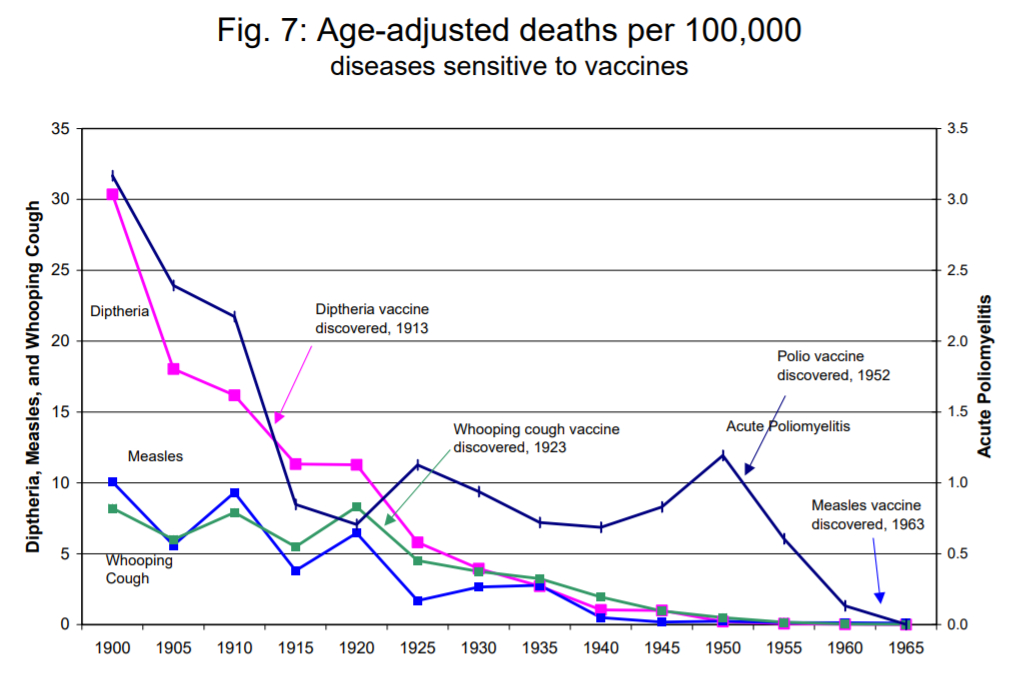
Cochrane and WHO recognize Vitamin A deficiency as a risk factor for measles infection; plenty of evidence exists to support that Vitamin A supplementation can alleviate the seriousness of measles infections.
Hysterisis is the permanent change in a system due to a shift in another part of the system. When corporate liability was removed for injuries and death in 1986, corporate influence on decision-making by the US CDC, HHS and ACIP become so strong and pervasive that today (1/20/2019), we saw the US Surgeon General getting defensive on whether he was “pro-vaccine” enough. This shift need not be permanent; indeed, regulatory recapture is very much on the mind for environmentalists (EPA), patients with loved ones killed by fast-tracked medicine (FDA), and, of course, the ever-increasing army of Vaccine Risk Aware Americans (CDC, FDA, NIAID).
Clearly, there is an end point to the measles mortality hysteresis, and clearly, these actualizations thus far are insufficient to reconcile public health public policies with reality. However, it seems the financial cost of denialism will be its own undoing.
Minnesota, USA: Vaccine Risk Denial Comes Home to Roost
The type of denial that has taken place is now coming back to bite states in their pocketbook. Anne Dachel, of Age of Autism, has been chronicling the soaring costs of special education programs in the website Loss of Brain Trust (https://www.lossofbraintrust.com) which now has thousands of media stories showing that society cannot keep up with the burgeoning cost of caring for kids with developmental disorders – and that States are turning their back on the families who need the assistance, after telling them that vaccines do not cause autism, ADHD, dyslexia, language delay and other forms of developmental disorders.
Anne Dachel’s Message
Anne sent a message focused on Minnesota. She recalled that ten years ago, the statistic of 1 in 32 Somali children with autism in Minnesota shocked the world. The state had assured the public that vaccines were not a cause of autism.
Now, in January 2019, Minneapolis Star Tribune reports that Minnesota schools are facing ‘crisis level’ in special education funding. From the Star Tribune article:
“School administrators say the
mandate’s growing financial burden is threatening their ability to
provide the same for all students.
Soaring special education costs are
squeezing the budgets of Minnesota schools — and quickly becoming school
districts’ top priority for the new legislative session.
While public schools are required to
provide special education services, federal and state governments cover
only a portion of the cost. That means Minnesota districts must dig in
their budgets, pull out money they would otherwise spend paying teachers
or remodeling aging buildings, and collectively fill in a gap that this
year is expected to balloon to $724 million.
For many districts, that exercise has
become increasingly painful, resulting in teacher layoffs, program cuts
and swelling class sizes. School administrators are quick to note that
they cannot — and would not — deny special education students their
right to an education that meets their needs, no matter the cost. But
they say the mandate’s growing financial burden is threatening their
ability to provide the same for all students.
“Districts are taking ever-increasing
amounts of money out of their general education funds to pay for special
education costs,” said Brad Lundell, executive director of Schools for
Equity in Education, a group that represents nearly 60 districts across
the state. “And that, I think, is reaching a crisis level in the state.”
Many school administrators and
advocates say the problem begins with the federal government, which has
never followed through on its decades-old pledge to cover 40 percent of
special education costs. Currently, the federal government pays for
about 8 percent of Minnesota’s $2.2 billion annual special education
expenses.
The share of the cost picked up by the
state has ticked up in the last decade, rising to about 63 percent this
year. But it’s not enough: more Minnesota students are requiring
special education services, including a growing number with particularly
complex medical, mental health or behavioral needs. The cost to serve
them is rising at a faster rate than the overall costs of education, and
the federal government isn’t responding in kind. …
“I would say this is probably the No. 1
issue for us from a budgetary standpoint,” said superintendent Wayne
Kazmierczak. “From a standpoint of what financially keeps us awake at
night, it certainly keeps us awake.” …
All told, Minneapolis has the state’s
largest special education funding gap: $55.3 million, or about $1,400
for every student in the district.
Anne’s past articles on Age of Autism from 2008 (here and here) and 2013 are now prescient warning unheeded. She is justifiably incensed in her message:“I was in Minneapolis when Somali leaders met with health/school officials for a public forum in 2008. Parents wanted answers. Education officials assured them that vaccines weren’t at fault AND THAT THE SCHOOLS WOULD PROVIDE FOR THEIR KIDS’ NEEDS.
NOW ….SPED costs are just too much to handle. Notice the photo on the story…….lovely little (I’m assuming Somali) girl, BUT NOT ONE WORD OF EXPLANATION AS TO WHY THERE IS THIS ‘GROWING NUMBER’ of disabled students more complex needs.
STILL…….they have to pretend the only problem is covering the cost–not why it’s happening. It’s something that just can’t continue.”
The acts of
pumping pregnant women and infants with neurotoxic metals, and citing
studies not designed to test causality as proof of a lack of causality
in the face of clear evidence of inappropriate scientific conduct at the
highest levels in CDC is best described as perseveration–
and the act of doing this same thing over and over and expecting a
different result it would seem, is not healthy for children and other
things.
In search of
confirmation of their bias, denialists also seize on the slightest
evidence to further dismiss the notion that vaccines do not cause
autism. For example, they cite MRI studies that have reported that
children with autism have significant early structural differences in
their brains compared to children without autism – and inappropriately
claim that such studies show that vaccines cannot cause autism – in
spite of the fact that such studies never considered the effects of
vaccines.
However, they
must forget that CDC shifted their position on vaccination during
pregnancy at the same time they ended the use of
thimerosal-containing vaccines (other than flu vaccines), and that the
infants being studied would have received aluminum from their
day-of-birth vaccination against Hepatitis B.
To me, the days of vaccine injury and denialism seem numbered. The
ploys advocated by the New York Times Opinion section carry a certain desperation – as do the efforts across the country to strip Americans of
their rights to religious, philosophical, and by social pressures such
as sanctions, medical exemptions.
Medical doctors in the US who choose to actually practice medicine
should not be penalized nor sanctioned for acting in good conscience on
these realities. It is utterly inconceivable that parents who choose to
exercise their legal rights to choose to skip some, or all, vaccines
for their children would be chastised. Remember, these events are
taking place in 2019 – an era in which HHS conceded in court to Robert F
Kennedy, Jr. and to Del Bigtree that they failed to comply with the
1986 law that required them to report, every two years, progress on
their attempts to make vaccines safer and to identify those at highest
risk of vaccine injury. (See ICAN’s new epic response calling HHS out for offering palliative responses to urgent and pressing questions).
If society really wants to eradicate measles, the actual efficacy
of the measles portion of the MMR must be determined via studies
conducted by entities with zero financial interest in the outcome of the
study. Why? Because Merck’s FDA-submitted efficacy data on mumps is
under intense scrutiny due to two whistleblowers who allege they were
forced to add rabbit antibodies [See Lawrence Solomon’s HuffPo article].
How can schools enforce mumps vaccination requirements when the
vaccine is being litigated as a potential mega-fraud? Why then should we
also trust Merck’s data on measles efficacy? If it as low as it might
be suspected, then the
number of vaccinated children in school with subclinical infections may
in fact vastly outnumber the vaccinated who are infected – making the contributed risk of new transmission chains from the unvaccinated miniscule. Since measles asymptomatic infection is real,
the path to measles eradication would involve in-home testing
requirements – and quarantine of individuals who have subclinical
infections. Ironically, the only way a school can learn of the
circulating subclinical infection may be to have a few unvaccinated
children who can show symptoms. Otherwise, immunocompromised children
could walk into a school teeming with silent, wild-type measles viruses
transmission chains among the vaccinated.
James Lyons-Weiler, PhD
Allison Park, PA
Comments