HPV vaccine from the angle of type replacement leading to increased cervical cancer rates
Below is a post from Dr. James Lyons Weiler on the topic of type replacement in HPV strains as a result of the HPV vaccine program. This is a different angle than the viral reactivation hypothesis that I posted yesterday. Most people have heard the expression nature abhors a vaccum. Dr. Weiler has written extensively on how by wiping out the established strains of HPV, the vacuum is filled by other strains of HPV that may also be oncogenic and maybe more oncogenic than the strains being eliminated.
OBJECTIVITY in science can be corrupted in the design, execution or interpretation of studies. In systematic reviews, and “official” government agency reports it can occur via similar mechanisms. A meta-analysis on the autism/vaccine hypothesis, for example, cited studies that had already been determined to be too flawed for inclusion in such considerations by the Institutes of Medicine, which rejected 17/22 studies. That IOM report itself cited 4 studies as valid that were in reality too low-powered to warrant inclusion. One study was so small that less than on person with ASD would be expected in one of the groups. The Polish study, with 96 vs 198 patients, found no association between vaccination with MMR and autism, but with such a small sample size, and it had too few patients enrolled to have sufficient statistical power. More on the issue of the reliance on low-powered studies to maintain a false safety profile for vaccines later.
Cochrane reviews have traditionally been respected as an example of objective, unbiased assessments of vaccine safety. They publish their review protocols ahead of execution, for example, and some of their reviews have bucked the mainstream mantra.
When it comes to their HPV Vaccine review, Cochrane apparently neglected to maintain independence. For example, during the planning of the protocol, they allowed a scientist from the CDC to participate in determining the design and scope of the review. This person, Dr. Markowitz, had also previously contributed to the scientific literature on the HPV vaccine, specifically on the question of whether the introduction of the vaccine to the market may be contributing to a shift in the prevalence of HPV types.
Here is what an unbiased Cochrane review would have reported, and the absence of this information causes me to lose all confidence in Cochrane as an objective, independent research entity:
“(1) Clinical studies of Gardasil used an invalid placebo, and therefore risk of adverse events due to the vaccine itself has not been determined. There is also evidence of deception on the part of Merck on the FDA report because they combined patients receiving saline and adjuvant (AAHS) placebo into one comparative group. The FDA has been notified of this and other unusual steps in the Merck studies, and has not issued any statement of concern nor called for action by Merck for remedy.
(2) The HPV vaccine short-term safety studies were funded by Merck. Those performing the studies had conflicts of interest, and therefore the decision to place conditions that developed after vaccination into ‘New Medical Condition’ files is a serious potential source of bias. Those data should be independently analyzed by scientists with no financial relationship to Merck, the US CDC, or any other agency, company or entity with a financial stake in the HPV vaccination program.
(3) Many of the studies have reported efficacy of the vaccine at reduce rates of CIN2+ lesions associated with HPV vaccine targeted types, but then draw unwarranted generalized conclusions about efficacy that can mislead the public.
(4) Many studies have concluded that rarer, potentially oncogenic, and oncogenic types do in fact replace the vaccine-targeted types, which are more common. The design and execution of CDC study (Markowitz et al., 2016) suffers from fatal flaws that could be interpreted as steps to obfuscate and hide type replacement. Specifically, the use of multiple independent univariate tests per HPV type rather that tests such as ANOVA resulted in small effect sizes in the shift in prevalence per type. A re-analysis of the total shift in vaccine-targeted on non-targeted types shows that the CDC study supports the conclusion that HPV vaccination does lead to type replacement.
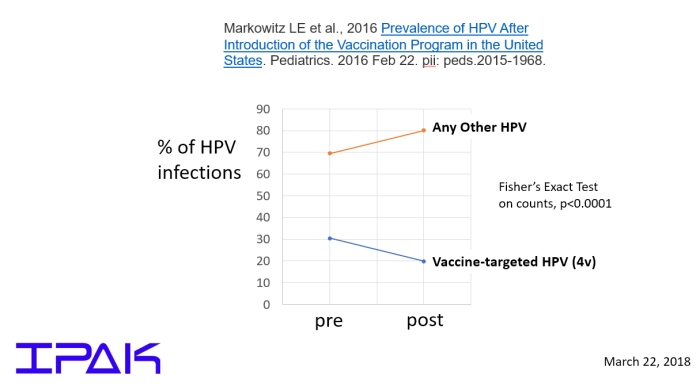 Figure 1. Re-analysis of Markowitz et al data focus on whether
non-vacccine-targeted types as a whole increased after the HPV 4-valent
vaccine was brought to market. Clearly the reduction of the
vaccine-targeted types results in an increase in the non-vaccine
targeted types. These results are based on counts, not percentages.
Figure 1. Re-analysis of Markowitz et al data focus on whether
non-vacccine-targeted types as a whole increased after the HPV 4-valent
vaccine was brought to market. Clearly the reduction of the
vaccine-targeted types results in an increase in the non-vaccine
targeted types. These results are based on counts, not percentages.
In spite of being informed of the flaw in the Markowitz et al. study, CDC has continued to cite the study as evidence that type replacement does not occur. However, given the findings of many other studies, the possible effects of the vaccination program could include a rise in rarer, potentially more lethal HPV types, including an increase in overall HPV-related cancers and deaths due to HPV-related cancers. A meta-analysis of studies of type replacement arbitrarily failed to consider studies with results that support the conclusion that type replacement is occurring.
(5) In contrast to conclusions drawn and statements made in some studies, by some government agencies, by many medical professionals, by medical organizations and by the press, there is no evidence that the HPV vaccine reduces the population-wide rate of cervical cancer, or any other type of HPV-associated cancer.
The combined effects of these circumstances forces the unfortunate, but real, conclusions that
(1) No credible science supports the claims of health benefits from HPV vaccination at the population level, and
(2) The risks of serious and moderate adverse events may be knowable via re-analysis of data submitted to the FDA for Gardasil 4-valent vaccine, and for the Gardasil 9-valent vaccine. However, at this time, no credible science exists that can support the conclusion that HPV vaccination is generally safe.
New randomized clinical trials with saline placebo are needed in which all new medical conditions are analyzed as potential serious adverse events. It is scientifically unsound to exclude medical conditions that emerge after vaccination due to assessment by those running the study that the conditions were not caused by the vaccine. The data should be allowed to speak for themselves.”
So why did Cochrane fail to come to these conclusions? One issue is that while her name is not on the final report, as an CDC scientist Markowitz was involved in the design of the protocol and, according to the report:
“We acknowledge Lauri Markowitz for her invaluable advice and contributions by reviewing the results and discussion sections.”
I had emailed Dr. Markowitz long ago and informed her that the CDC study supported type replacement by pointing to their own result: no net change in total HPV infection rates before, and after, the vaccine was brought to market. I also informed her of the existing studies that pointed to type replacement. In other words, she knows. It is therefore remarkable – and telling – that the Cochrane report did not even mention type replacement.
The other issue is that Cochrane now receives funding from the Bill and Melinda Gates Foundation. See AHRP: Gates Foundation Buys Cochrane Integrity for $1.15 Million.
The media has in multiple places misrepresented the report, perhaps due to its misleading title. To help, here is a major result from the Cochrane report:
“Cervical cancer outcomes are not available.”
and a major conclusion:
“Long-term of follow-up is needed to monitor the impact on cervical cancer, occurrence of rare harms and pregnancy outcomes”.
In other words, it is premature and incorrect to say “HPV Vaccines Prevent Cervical Cancer”.
I have seen posts on social media to the effect of “objectivity in science is dead”, to which I reply:
“Ahem”.
OBJECTIVITY in science can be corrupted in the design, execution or interpretation of studies. In systematic reviews, and “official” government agency reports it can occur via similar mechanisms. A meta-analysis on the autism/vaccine hypothesis, for example, cited studies that had already been determined to be too flawed for inclusion in such considerations by the Institutes of Medicine, which rejected 17/22 studies. That IOM report itself cited 4 studies as valid that were in reality too low-powered to warrant inclusion. One study was so small that less than on person with ASD would be expected in one of the groups. The Polish study, with 96 vs 198 patients, found no association between vaccination with MMR and autism, but with such a small sample size, and it had too few patients enrolled to have sufficient statistical power. More on the issue of the reliance on low-powered studies to maintain a false safety profile for vaccines later.
Cochrane reviews have traditionally been respected as an example of objective, unbiased assessments of vaccine safety. They publish their review protocols ahead of execution, for example, and some of their reviews have bucked the mainstream mantra.
When it comes to their HPV Vaccine review, Cochrane apparently neglected to maintain independence. For example, during the planning of the protocol, they allowed a scientist from the CDC to participate in determining the design and scope of the review. This person, Dr. Markowitz, had also previously contributed to the scientific literature on the HPV vaccine, specifically on the question of whether the introduction of the vaccine to the market may be contributing to a shift in the prevalence of HPV types.
Here is what an unbiased Cochrane review would have reported, and the absence of this information causes me to lose all confidence in Cochrane as an objective, independent research entity:
“(1) Clinical studies of Gardasil used an invalid placebo, and therefore risk of adverse events due to the vaccine itself has not been determined. There is also evidence of deception on the part of Merck on the FDA report because they combined patients receiving saline and adjuvant (AAHS) placebo into one comparative group. The FDA has been notified of this and other unusual steps in the Merck studies, and has not issued any statement of concern nor called for action by Merck for remedy.
(2) The HPV vaccine short-term safety studies were funded by Merck. Those performing the studies had conflicts of interest, and therefore the decision to place conditions that developed after vaccination into ‘New Medical Condition’ files is a serious potential source of bias. Those data should be independently analyzed by scientists with no financial relationship to Merck, the US CDC, or any other agency, company or entity with a financial stake in the HPV vaccination program.
(3) Many of the studies have reported efficacy of the vaccine at reduce rates of CIN2+ lesions associated with HPV vaccine targeted types, but then draw unwarranted generalized conclusions about efficacy that can mislead the public.
(4) Many studies have concluded that rarer, potentially oncogenic, and oncogenic types do in fact replace the vaccine-targeted types, which are more common. The design and execution of CDC study (Markowitz et al., 2016) suffers from fatal flaws that could be interpreted as steps to obfuscate and hide type replacement. Specifically, the use of multiple independent univariate tests per HPV type rather that tests such as ANOVA resulted in small effect sizes in the shift in prevalence per type. A re-analysis of the total shift in vaccine-targeted on non-targeted types shows that the CDC study supports the conclusion that HPV vaccination does lead to type replacement.
In spite of being informed of the flaw in the Markowitz et al. study, CDC has continued to cite the study as evidence that type replacement does not occur. However, given the findings of many other studies, the possible effects of the vaccination program could include a rise in rarer, potentially more lethal HPV types, including an increase in overall HPV-related cancers and deaths due to HPV-related cancers. A meta-analysis of studies of type replacement arbitrarily failed to consider studies with results that support the conclusion that type replacement is occurring.
(5) In contrast to conclusions drawn and statements made in some studies, by some government agencies, by many medical professionals, by medical organizations and by the press, there is no evidence that the HPV vaccine reduces the population-wide rate of cervical cancer, or any other type of HPV-associated cancer.
The combined effects of these circumstances forces the unfortunate, but real, conclusions that
(1) No credible science supports the claims of health benefits from HPV vaccination at the population level, and
(2) The risks of serious and moderate adverse events may be knowable via re-analysis of data submitted to the FDA for Gardasil 4-valent vaccine, and for the Gardasil 9-valent vaccine. However, at this time, no credible science exists that can support the conclusion that HPV vaccination is generally safe.
New randomized clinical trials with saline placebo are needed in which all new medical conditions are analyzed as potential serious adverse events. It is scientifically unsound to exclude medical conditions that emerge after vaccination due to assessment by those running the study that the conditions were not caused by the vaccine. The data should be allowed to speak for themselves.”
So why did Cochrane fail to come to these conclusions? One issue is that while her name is not on the final report, as an CDC scientist Markowitz was involved in the design of the protocol and, according to the report:
“We acknowledge Lauri Markowitz for her invaluable advice and contributions by reviewing the results and discussion sections.”
I had emailed Dr. Markowitz long ago and informed her that the CDC study supported type replacement by pointing to their own result: no net change in total HPV infection rates before, and after, the vaccine was brought to market. I also informed her of the existing studies that pointed to type replacement. In other words, she knows. It is therefore remarkable – and telling – that the Cochrane report did not even mention type replacement.
The other issue is that Cochrane now receives funding from the Bill and Melinda Gates Foundation. See AHRP: Gates Foundation Buys Cochrane Integrity for $1.15 Million.
The media has in multiple places misrepresented the report, perhaps due to its misleading title. To help, here is a major result from the Cochrane report:
“Cervical cancer outcomes are not available.”
and a major conclusion:
“Long-term of follow-up is needed to monitor the impact on cervical cancer, occurrence of rare harms and pregnancy outcomes”.
In other words, it is premature and incorrect to say “HPV Vaccines Prevent Cervical Cancer”.
I have seen posts on social media to the effect of “objectivity in science is dead”, to which I reply:
“Ahem”.
Comments